
The Gender Identity Takeover of the Royal College of GPs

In October 2024, I wrote about the ways in which internal activist doctors and gender lobby groups Gendered Intelligence and Stonewall have been allowed to have unfettered influence over the Royal College of Paediatrics. The extent of this was shown by the college giving Gendered Intelligence an article advertising its services in the national magazine for paediatricians in Spring 2023. This article encouraged paediatric doctors to support social transition for child and adolescent patients, going against the recommendations of the Interim Cass Review. It also stated that these patients should be allowed to be accommodated in opposite sex spaces within hospitals.
Unfortunately, internal activists and external gender lobby groups have also had an incredible amount of influence over several other medical royal colleges in the UK. One of these is the Royal College of GPs, which is for doctors who often have the first contact with patients in their medical journey. In light of the news that the current government has recently announced that it is permanently banning puberty blockers, the Royal College of GPs’ historical and current stance on the topic of ‘gender identity’ is troubling.
The Affirmation Only Memorandum of Understanding
Many people will not be aware that the Royal College of GPs signed and remains a signatory of the contentious ‘Memorandum of Understanding on Conversion Therapy in the UK Version 2’, which states that ‘[demonstrating] an assumption that any [...] gender identity is inherently preferable to any other’ and trying to change this is conversion therapy and should be prohibited. The problem with this line of thinking is that so-called ‘gender identity’ has no evidence base for being a fixed and inherent aspect of a patient and many argue that the concept is based solely on sex stereotypes. It also means that GPs have been signed up to the idea that they cannot disagree with medical harm for patients based upon ‘gender identity’ and must prioritise this internal status over the physical body.
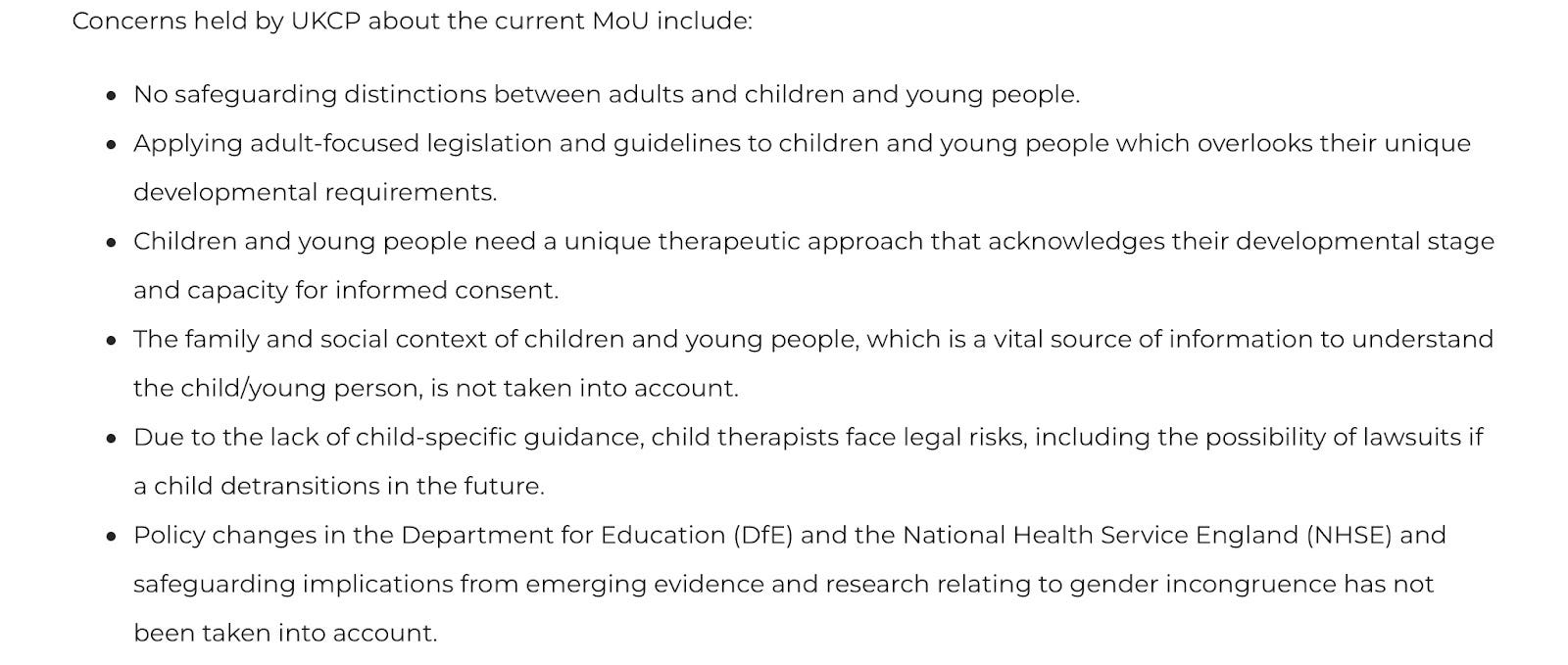
Concerns around safeguarding issues for children and adolescents recently led the counselling body the UK Council for Psychotherapy (the UKCP) to withdraw their signature from this Memorandum of Understanding. In April 2024, the UKCP stated ‘The current MoU was drafted to apply to adults and was retrospectively applied to children and young people without consultation with the relevant bodies and child therapists with the specialist and regulatory knowledge of working with children and young people’. The UKCP goes on to cite the MoU’s failure to consider children’s needs based on their stages of development and their lack of ability to give informed consent. It also describes the risk of future lawsuits for its members should it remain signed up to this, alongside the fact that emerging evidence increasingly contradicts the MoU.
Considering the above, it is shocking that many major medical and counselling organisations remain signed up to the Memorandum of Understanding, which attempts to ban any questioning of a patient’s gender identity. As shown in the screenshot below, this includes the Royal College of GPs, NHS England, NHS Scotland, the British Psychological Society and all main counselling organisations other than the UKCP.

It is interesting to note, however, that the National Counselling Society (now the NCPS) also removed their signature from this Memorandum of Understanding for a period of time. In April 2024, the gender activist group Therapists Against Conversion Therapy and Transphobia (TACTT) expressed objections upon discovering that the NCPS appeared to have quietly removed their signature from the MoU at the start of 2023. The Psychotherapy and Counselling Union also called the NCPS’s withdrawal from this MoU ‘disgraceful’. Although communication from the NCPS stated that the removal of their signature had been due to being named in legal action, by May 2024 they had reinstated their signature on this Memorandum of Understanding to ban questioning their clients’ ‘gender identities’. This is an action that seems to have been taken in response to these gender activists’ demands.
Considering the fragile legal status of this Memorandum of Understanding and its concerning approach to safeguarding, it is astonishing that major organisations such as NHS England, NHS Scotland and the Royal College of GPs remain signatories. It is also noteworthy that gender identity lobby groups are involved, such as Gendered Intelligence (whose links to the Royal College of Paediatrics I previously mentioned) and GLADD UK.
GLADD UK is the Association of LGBTQ+ Doctors and Dentists that wrote the national medical schools charter which states that doctors and medical students must ‘affirm [patients’] gender identity’ and provide ‘joyful’ depictions of ‘LGBTQ+’ patients. Despite the clear safeguarding risks of doctors being required to automatically affirm all patients’ self-diagnosed ‘gender identities’ for which they would like medical interventions, 80% of UK medical schools have signed this charter. I described further worrying aspects of this charter in my article A Gender Critical Analysis of GLADD’s Affirmation Only Medical Schools Charter.
Gender Lobby Groups Providing GP Training
GIRES
Besides its continued agreement with the Memorandum of Understanding that its GP members will not question patients’ ‘gender identity’, the Royal College of GPs’ LGBT training has also been influenced by gender lobby groups for some time. In 2013, the Gender Identity Research & Education Society (GIRES) wrote e-learning for the Royal College of GPs and all GPs on ‘gender variance’ in patients. GIRES is a charity which states that it ‘empowers and gives a voice to trans and gender diverse individuals, including those who are non-binary and non-gender. We use evidence from individuals’ lived experiences, combined with scientific research into gender identity development, to educate all those who are able to improve trans and gender diverse individuals’ wellbeing. We contribute to policy development regarding equality and human rights for individuals, especially in healthcare. We also deliver training, e-learning and information to public and private sector organisations’.
For a period of time, this means that the LGBT training for all GPs on so-called gender variance was being written by an activist lobby group basing this on ‘lived experience’ (or personal anecdote) regarding patients’ self-diagnosed ‘gender identity’. The implication that there is any scientific evidence base to the concept of ‘gender identity’ from this group is also highly questionable.
Interestingly, a rift appears to have taken place between GIRES and the Royal College of GPs in 2019. At this point, the e-learning written by GIRES was removed after a disagreement between the two organisations due to changes that the RCGP made to this with which GIRES disagreed.
GIRES provided a statement in February 2019, specifying that ‘On 30 January 2019, [GIRES] removed the Gender Variance e-learning course from the Royal College of GPs website. This was because The RCGP had without prior warning made unauthorised changes to the content of the course for which GIRES owned the copyright. Some of those changes undermined the responsibility of GPs, as stated by NHS England and the General Medical Council, to prescribe and monitor the medication recommended by the specialist clinicians in the gender identity clinics. The RCGP was unwilling to reverse those changes. Both parties decided that the course should be removed from the RCGP website.’
Mermaids
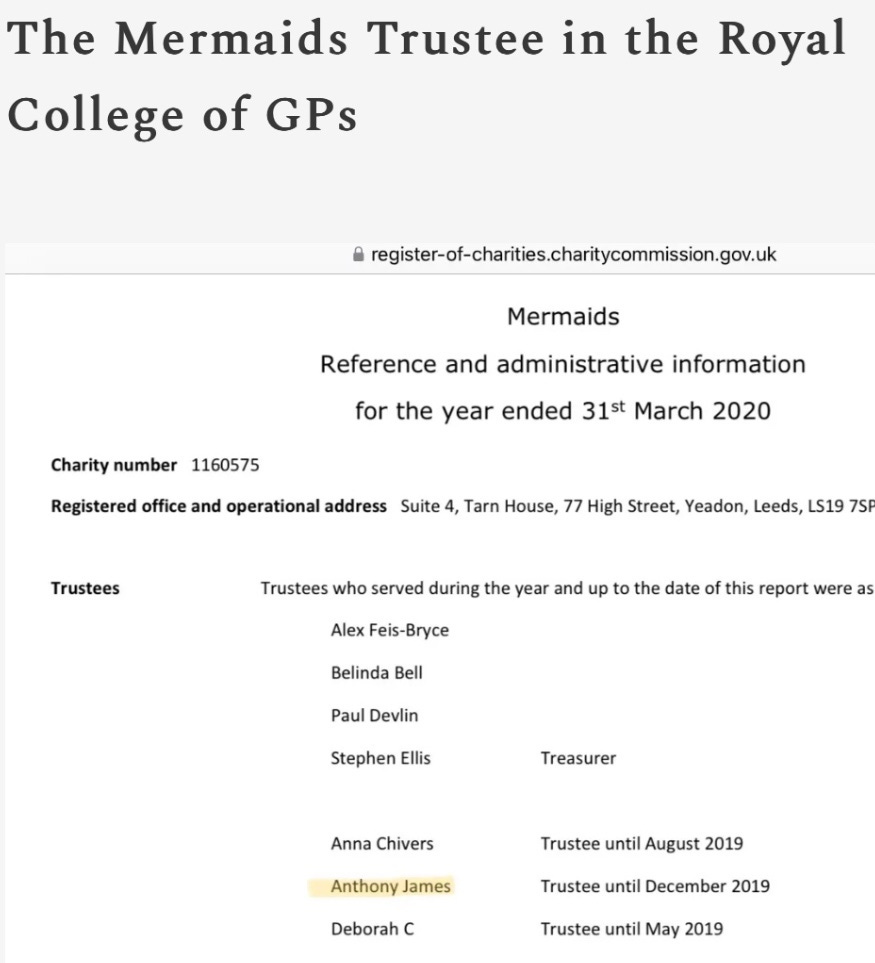
However, although GIRES stopped their collaboration with the Royal College of GPs in 2019, that same year a doctor who was also a trustee of Mermaids wrote LGBT education for all UK GPs due to his high up roles in the college. This was Dr Anthony James, husband of Pink News founder and CEO Benjamin Cohen. As I have previously described, this doctor could also be said to have had a conflict of interests in that his household gained substantial income from Pink News’ advertising of medical ‘gender transition’ to children and teenagers via their Snapchat shows, such as Pure Trans Joy. In 2022, the majority of Pink News’ revenue stream came from Snapchat (as reported by the Press Gazette).
Dr Anthony James wrote this LGBT education for all GPs in collaboration with the Government Equalities Office and this was published in January 2020. Dr James only stepped down from his role as a Mermaids trustee in December 2019, so was involved in this organisation while working with the Government Equalities Office to create guidance for all GPs via their royal college.
Before that, in 2018, Dr James organised for Susie Green and other members of the charity Mermaids to directly teach GP trainees. The public is largely unaware of the involvement that this disgraced charity has had in GP training. It is alarming that the population has had no knowledge or say in gender identity lobbyists being able to directly influence the taxpayer-funded NHS. This was also despite Mermaids’ insistence in one court case that it does not ‘do medical stuff’.

These examples are not exhaustive and there are many other gender identity lobby groups who have also appeared to influence the Royal College of GPs. Going forward, NHS organisations’ use of external groups must be completely transparent to the public. The ideological steering that these groups have been allowed to have over medical royal colleges and other groups within the NHS cannot be underestimated.
Thank you for this.
I work in the medical industry and certain things have always puzzled me about the capture of my otherwise sensible peers.
Imperative that medicos learn the information in this excellent article.
Imperative your information is delivered way more broadly than just this platform.
Imperative that this is stopped.
Or countered with equally passionate education to support the science that actually represents true 'best practice' to support a patient's 'best outcome', with evidence backed up by 'true case studies', or better yet, people who have been harmed already by this appalling medical practice.
Using the words 'gender critical', or 'anti- trans' immediately sets medicos- caring intellectuals at best- on the defence of the marginalised.
Better to deliver it as 'Best Practice science'/'best outcome' science.
In the same way Total Knee Replacements are delivered in a safe, economically viable and timely manner. With a 'watch and wait' protocol that delivers surgery only when the risk of surgery is met by the loss of function/ ability to walk.
When the patient is less likely to need a second replacement, at an age where the wearing out of the new prosthesis is less likely, hence decreasing the risks associated with surgery by AVOIDING UNNECESSARY SURGERY.
No doctor argues with that!
Knee pain patients are sent to the Orthopoedic specialist after MANY, many visits to the GP, and YEARS and years of referrals to physiotherapists, BEFORE being to be sent to an orthopoedic specialist.
Who in turn knows the risks of surgery and avoid it at all costs.
And if he or she needs to address the problem with surgery, they do so at least resort, and in a way to minimise the chance of ever having to do repeat surgery.
This is not argued.
Young doctors do not argue with their superiors when patients attend in pain, begging for a knee replacement.
Now I understand better why my young colleagues move past their timidity to speak up against their mentors when it comes to this ideology.
Young doctors (essentially many were marginalised by things including high iq, vulnerable, biased against, bullied as children, autistic, raised in florin countries etc etc) who are ripe for having their naive, sheltered, caring natures taken advantage of, are already being trained to be flying monkeys for the pharmaceutical industry.
They are trained to exhaustion, have no space for reflection, let alone to study information outside anything that will be on an exam, or delivered in sponsored lunch meetings that offer only a chance to sit, breathe for a moment and eat nutritious, tasty food provided by sponsors while the sponsors speak.
These tender, naive 'kids' who will become doctors, are sitting ducks for mass recruitment toward the definite harm of affirmative care.
This is DANGEROUS.
And appalling.
This is direct, state funded abuse on a massive scale.
I listened to Andrew Gold's interview of Andrew Wallis of 'Unseen'.
What's happening with this addition to medical training, is just like all the limos waiting outside the orphanages, in the country where state funding for orphans ceases at a certain age. The kids come out, are seduced with golden promises into the waiting cars, and taken to a trapped future of bondage and slavery.
Except this is WORSE.
Happening in the bright light of day, in plain sight, funded by governments, actively targeting the vulnerable in an extreme abuse of power, orchestrated by mass marketing (internet access- not just social media- captures the insecurities of minors), delivers the vulnerable person- by direct concern of sincere caregivers- to the help they think they will receive.
Instead, are captured in an imbalance, where the doctor's revered knowledge is bowed down to.
If the GP has any quiet doubts or pangs of intuition,
the capture is often enhanced by the GP's quick google on the RCGP website's page 'management of gender dysphoria'.
Where a tidy list of 6 steps, gives the time-pushed GP a quick way to get the patient's concerns addressed quickly, in a way that addresses the GP's conscience. Either a referral to a paediatrician follows (where the above process is repeated) and a referral to the gender specialist clinic, satisfies both the GP and paediatrician's consciences.
And they are done.
This process either separates the vulnerable minor from the equally vulnerable caregiver, by browbeating the carer to conform to the 'greater knowledge' of the all- knowing medico, or justifying the removal of the carer who knows their child better and listens to their intuition rather than following the doctor's advice. Which doesn't go down well if it is done openly.
This
Is
Horrifying.
When was the teaching of ethics removed from the medical training syllabus? Hippocrates must be spinning.: https://lucyleader.substack.com/p/first-do-no-harm
What other illness, condition or whatever is accepted without question on the basis of self-diagnosis? Women die of ovarian cancer because GPs don't take their pain and symptoms seriously, but a 10-year-old is believed when (they have been indoctrinated) to declare they are in the wrong body?
"If you believe that even bodies aren’t factual, but are just complex social constructions, you have no business treating or advising others." https://lucyleader.substack.com/p/um-yes-this-is-interesting-but-how